
How many phantoms can haunt a building at once? When the building is a psychiatric hospital, the answer is complex; even more so when it is one of the 78 “linear plan” asylums built during the second half of the 19th century according to principles established by the American physician Thomas Story Kirkbride. 1 Innovative in design and beneficent in intent, these hospitals were meant to facilitate the patient-centered practices of moral treatment, rooted in Enlightenment science and spiritualism. 2 Typically funded and managed by states as public institutions, they reflected the values of the society from which they emerged, and which they shaped in turn.
Yet disturbing histories and phantoms of many kinds have gathered around these buildings, presenting challenges for their preservation and reuse. No one essay can make a full accounting; however, I will examine some of the forces — social, political, medical, architectural — that led to the neglect of these buildings, the demolition of more than half of them, and to a more general disregard for the mental health of Americans over the past century and today. 3 I will also consider alternate histories that might have occurred if certain defining events had played out differently. But first I’d like to introduce you to my grandparents, Earle and Beatrice Kirkbride.
Origins
Earle Rosslyn Kirkbride was a painter and golden-age illustrator for books and magazines, who died when I was just over one year old. I inherited his indestructible blue jacket, which has an indelible mark of Van Dyke Brown paint on its right-hand pocket that was likely picked up while he was working in his studio on the second floor of 704 South Front Street, Philadelphia — the 1762 brick rowhouse that he and my grandmother bought and restored in the 1950s. Whenever I visited her there, which was often, I slipped off to his studio, preserved exactly as it was when he died; pungent with turpentine and linseed oil, and packed with his oil paintings, aquatints, sketches, and tools. One canvas, set on Earle’s massive oak easel, fascinated me. Titled The Welcome, the painting depicts Tamanend, “the affable one,” sachem of the Turtle Clan of the Lenni-Lenape nation, who stands on the western bank of the Lenapewihittuk, also known as the Delaware River. His back to the viewer, Chief Tamanend gazes out at a ship bearing William Penn and other members of the Society of Friends, who had made a lengthy and difficult voyage from England, in 1682. Their ship was named The Welcome, and one third of its passengers had died of smallpox on their transatlantic journey to found the Quaker colony of Pennsylvania and its capital city, Philadelphia.
‘I’ve come to realize there were lots of bugs in the illustrations I made for those American history books,’ wrote Earle R. Kirkbride.
My young mind absorbed two haunting impressions from this painting. First, it fascinated me precisely because it was almost, but not quite, finished. My grandfather’s intentions were clear, based on studies in different media, but his version in oils would remain forever incomplete, a fact that awakened in me a melancholy awareness that we all run out of time someday, and our works may remain only partially realized. Second, I was captivated by its unusual point of view. Rather than centering the composition on Penn, Earle placed the observer among the Lenni-Lenape on the river’s bank, witnessing the colonists’ arrival from a step or two behind the right shoulder of Tamanend, whose posture conveys a hint of apprehension. 4 Reputedly, the chief and Penn established a peace that was unique among the colonies — “the only treaty never sworn to and never broken,” Voltaire said — yet I had also learned that the Quakers proved inconsistent in their friendship with the Lenni-Lenape. 5 The Welcome provided an uncanny perspective, filling me with ambivalence about my origins.

Through my grandfather, I am a direct descendant of Joseph Kirkbride, who made a similar journey on a different ship, The Bristol Factor, arriving ten months in advance of this scene. Joseph was a Quaker, too, from Kirkbride, England, a few miles from the west end of Hadrian’s Wall. These kinds of details were significant to my grandmother, whose own Quaker family had originated near the east end of the Wall. Through the research and rehabilitation of that rowhouse, Beatrice emerged as an architectural historian, preservationist, and civic activist. She successfully applied to have 704 South Front listed on the National Register of Historic Places and protected with two adjacent structures in a National Historic District. 6 For several decades Bea investigated the history of colonial neighborhoods and buildings with the Philadelphia Historical Commission, establishing several National Historic Landmarks. 7 She and my grandfather also fought a long-running battle against the Philadelphia Planning Commission and the state Department of Highways, opposing the construction of an I-95 exchange along the waterfront and a “Crosstown Expressway” (I-695) that would have demolished an African American neighborhood and several blocks of South Front Street. “Thanks to all the research work Beatrice has been doing,” Earle confided in 1959, “I’ve learned more about colonial days than I ever knew before, and I’ve come to realize there were lots of ‘bugs’ in the illustrations I made for those American history books.” 8 Their combined efforts, as detective and artist, contributed to the eventual cancellation of the Crosstown Expressway. 9
What he had in mind was a reimagining of episodes in the colonial Quaker story, to make its phantoms apparent.
In tandem with this campaign, Earle worked on a project he called The Phantoms & Ghosts of the Holy Experiment, a “portfolio of paintings” that reflect on the promise and contradictory consequences of Penn’s vision for Pennsylvania as a haven for Quakers and other persecuted minorities — a “Holy Experiment” based on ideals of pacifism, religious tolerance, and egalitarianism, unified through landscape and city planning. 10 In his close readings of historical sites in Philadelphia, my grandfather perceived conflicting undercurrents within this experiment. 11 “I believe God has visualized for me what I have so long worked at,” he wrote. “I am not well; and fear my time may run out before I have finished the job. I hope I do not hurry thru the end. That it may be finished and the end quick.” What he had in mind was a reimagining of episodes in the colonial Quaker story, to make its phantoms apparent. “As Rembrandt depicted himself and his family and his friends and his immediate surroundings and people of his time, in the knowledge of myself I must go back and visualize with whatever help I can find the actual place and people (relatives) and whatever they do as living people in local (surroundings) here in America and back in England and beyond if possible.” 12 In these artworks, he depicted scenes from the Quaker experiment, populated with ghostly characters (including historical figures identified in handwritten notes), and combined them with snapshots of mid-20th century life in Philadelphia, during a period of extreme social upheaval and destructive urban “renewal” in that city and across the United States.

Twelfth Street Friends Meeting House and PSFS Building, pencil drawing by Earle R. Kirkbride, 1961. The ancillary building at the left served as the headquarters for the American Friends Service Committee Council, representing pacifist conscientious objectors, formed after World War I. For their humanitarian efforts during World War II, the AFSCC and its British counterparts received a Nobel Peace Prize, in 1947.

Cover page design for Phantoms & Ghosts of the Holy Experiment: a Portfolio, line drawing by Earle R. Kirkbride, 1956.
Holy Experiment from Front Street Southwark, etching by Earle R. Kirkbride (1957). A view of center city Philadelphia from a rear window at 704 South Front Street, including, in the distance, a statue of William Penn atop City Hall, next to the pinnacle of the PSFS Building. This etching was featured in the Philadelphia Sketch Club’s 1959 calendar, with this caption: “The ‘Holy Experiment’ of William Penn to create a city of order and green trees has gone somewhat awry in the sprawling growth of Southwark as Mr. Kirkbride depicts. The needs of commerce and the expansion of the city have crowded out all semblance of Penn’s dream.”
Scale figures (Beatrice and Edward Kirkbride) at a vacant site adjacent to the Free Quakers Meeting House, photographed by Earle R. Kirkbride, 1961.
Free Quakers Meeting House, oil painting by Earle R. Kirkbride, 1961. Inherent tensions between worldly governance and Quaker principles of non-violence emerged in the mid-18th century. During the French and Indian War, Quaker representatives were compelled to withdraw from the Pennsylvania Assembly so that a militia could be formed. Later, during the American Revolutionary War, Quaker members who took up arms against the British were formally expelled from the Society of Friends. Some of them formed a splinter group, the Free Quakers Society, whose name is reflected in the title of this painting.
Free Quakers Meeting House, detail. Ghostly figures including Thomas Jefferson, Benjamin Franklin, and George Washington occupy the current-day palimpsest of a residential rowhouse adjacent to the Free Society’s Meeting House at 5th and Arch Streets.
700 Block South Front Street, oil painting by Earle R. Kirkbride, 1961-65, featuring a late 18th century street scene.
700 Block South Front Street, detail, highlighting Earle gazing out from his artist studio on the second floor of 704 South Front.
Front page of The Philadelphia Inquirer, January 3, 1965, featuring a line drawing of 700 Block South Front Street, by Earle R. Kirkbride.
Dedication of the Thomas Story Kirkbride Building at Byberry State Hospital, Philadelphia, on July 31, 1980, with Beatrice H. Kirkbride (second from right) and Anna Kirkbride Shaudys (right). Photographer unknown.









Earle’s project brings us back to Dr. Thomas Story Kirkbride, the visionary force behind those 78 psychiatric hospitals. He, too, was a direct descendant of Joseph Kirkbride, on a branch parallel to my grandfather, hence a distant cousin. One of the drawings in the Phantoms & Ghosts series depicts the Friends Meeting House where Dr. Kirkbride was a lifelong member, and where his funeral service was held. Originally constructed in 1755 at Second and Market Streets, the building was disassembled in 1809 and diligently reassembled, board by board, at a new site on Twelfth Street, one mile from the Delaware River, at the center of Penn’s “Greene Countrie Town.” The financial powers of Philadelphia grew up around it, including the modernist skyscraper seen here. The PSFS Building was designed in 1932 by George Howe and William Lescaze for the Quaker-founded Philadelphia Savings Fund Society — the first savings bank in the United States. 13 My grandfather presented it from an unusual rear view, juxtaposed with the Friends’ Meeting at its base, suggesting his aim to capture the adjacency of purposes — and inherent tensions — between the Quakers’ spiritual pursuits and worldly endeavors. Similar tensions underlie the Kirkbride Plan hospitals.
The best kind of hospitals — not only best built, but with the most perfect arrangements and fixtures of every kind, and managed in the most liberal and enlightened manner — are sure to be most economical in the end.
— Thomas Story Kirkbride, 1854
The convergence of idealism and pragmatism in Dr. Kirkbride’s prose reflects the “curious blend of religious and scientific values” that imbued his conviction that insanity could be cured in carefully arranged settings. 14 He also shared with the early Philadelphia Quakers an abiding interest in architecture and landscaping. Having been ill-treated by authorities in England, the Friends were compelled to establish improved social and physical infrastructures for health and justice. 15 Following their belief that every living person — sane, insane, model citizen, or criminal — represents an “inner light” deserving respect, Quakers built hospitals and penitentiaries in the spirit of Penn’s Holy Experiment, with the aim of restoring and rehabilitating patients and penitents. 16 “Those who recover may become valuable citizens,” Kirkbride wrote of the mentally ill; “if they do not add directly to the wealth of the State, they at least support their families.” 17
Similar tensions — between the Quakers’ spiritual pursuits and their worldly endeavors — underlie the Kirkbride Plan hospitals.
An orthodox Quaker and aspiring surgeon, Kirkbride gained direct experience with the mentally ill as a resident physician at the Frankford (Friends) Retreat in North Philadelphia in 1832-33. 18 Featuring a central administration building with wings for patient rooms, set amidst pleasure grounds, Frankford embodied an underlying hygienic and spiritual concern for light and fresh air that became elemental to Kirkbride’s hospital planning. 19 After several years in private practice and a residence at Pennsylvania Hospital, where he had further opportunity to study mental disorders, in 1840 Kirkbride accepted an offer to become the first superintendent of the new Pennsylvania Hospital for the Insane, in West Philadelphia, a position he would occupy until his death, in 1883. 20 Although he did not contribute to the design of this particular building, he learned from its shortcomings, and he formed a bond with Samuel Sloan, the young architect who completed its construction and, in the years to come, would design over a dozen Kirkbride hospitals.
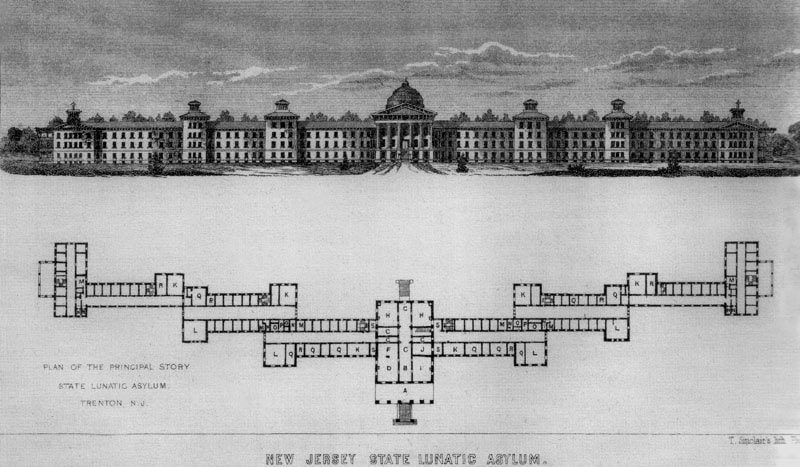

In October 1844, Dr. Kirkbride and twelve of his peers founded the Association of Medical Superintendents of American Institutions for the Insane (a precursor to the American Psychiatric Association) and elected Kirkbride as Secretary. 21 In articles published in AMSAII’s The American Journal of Insanity in 1847 and 1849, and in an early hospital built to his guidelines at Trenton, New Jersey, Kirkbride developed an idealized model of a residential facility to treat mental illness, generating a set of propositions that were adopted by AMSAII in 1851 and formed the basis for his 1854 treatise, On the Construction, Organization, and General Arrangements of Hospitals for the Insane with Some Remarks on Insanity and Its Treatment. In its 80 pages, Kirkbride offered a blueprint that influenced the rapid construction of dozens of facilities. 22
In an 1854 treatise, Thomas Story Kirkbride offered a blueprint that influenced the rapid construction of dozens of facilities.
The Linear Plan, as Kirkbride called his signature configuration, featured a central administration building flanked symmetrically by wings (one for women, the other for men), with shallow setbacks, in echelon, as seen in Sloan’s 1854 drawings for a state hospital at Tuscaloosa, Alabama. This v-shaped “batwing” arrangement provided light and air to disperse the miasma of foul odors, believed to be a primary source of illness. 23 The wings also structured daily life at the institution. 24 Patients were strategically distributed according to the nature and degree of their illnesses, with the most “excitable” cases placed in the outer wings. Patients closer to the Central Main building, where the superintendents often resided with their families, were closer to returning to the world.
The plan was continually modified to improve performance. At St. Elizabeths, in Washington, D.C. (1852) — the only federal facility built on the Linear Plan — the wing setbacks were deepened to allow for fireproof stairways and enhanced ventilation, natural lighting, and exterior views. With each hospital built over the following decades, the formal arrangements were adapted to meet site conditions and financial capacity, as well as advances in construction and technology. In 1880, Kirkbride published a second edition of his treatise, expanded to 341 pages and featuring the “Improved Linear Plan,” with bay-windowed communal spaces at the middle and outer end of each wing, and centralized rear support buildings. 25

Generous proportions were specified for all rooms, public and private. Patient rooms were to be at least eight by ten feet, with twelve-foot ceilings. Yet to prevent overcrowding, Kirkbride stipulated that they not be much larger than that, to forestall “two patients being placed in the same room, which ought not to be allowed.” Corridors were to be spacious and welcoming to promote social interaction — twelve feet wide in the wings, and sixteen in Central Main. 26
He was mindful of the psychological impact of physical spaces, promoting an overall openness and generosity that would reduce a patient’s sense of constraint and confinement.
According to Kirkbride, the role of a hospital architect was to ornament or style the physical envelope of the building — with “good taste,” yet not too “elaborate or costly” — while the operational layout and workings were determined by an experienced superintendent. Yet few superintendents could match Kirkbride’s experience or fluency in architecture. Consistent with his training as a physician, he “considered the workings of the hospital from a physiological perspective, attending to the natural flows of air and light and innovations in plumbing and heating, while also focusing on the flows of everyday life — the daily regimen of patients, doctors, and staff.” 27 He was mindful of the psychological impact of physical spaces, promoting an overall openness and generosity that would reduce a patient’s sense of constraint and confinement. Each room was to have internal ventilation and at least one window, whose security “should be masked, as far as possible, by arrangements of a pleasant and attractive character.” 28
The Kirkbride Plan generated elegant and voluminous structures that embraced local climate and site conditions, providing patients with fresh air, ample sunlight, and expansive vistas of bucolic, landscaped grounds, often including farms that provided food and opportunities for occupational therapy, with greenhouses, workshops, and other innovative infrastructures and amenities. A spacious “amusement room” was therapeutically and architecturally central. 29 Kirkbride believed lectures and theatrical performances would lighten patients’ moods, and he pioneered the use of “magic lantern therapy” to stimulate curiosity and mental healing. In a purpose-built hall, outfitted with benches and a podium for the lantern, patients could enjoy slide lectures on science, history and geography, including “The Life and Character of William Penn,” “Spencer’s Faerie Queene,” “Caves and Springs,” “The Life and Character of Joan of Arc,” “Morse’s Magnetic Telegraph,” and “The History of Pennsylvania.” 30 By 1857 there was a set program of 122 shows, “designed as a voyage starting in Philadelphia in the autumn, continuing to a different place each night and returning back to the hospital at the beginning of the summer.” 31

Dr. Kirkbride had a longstanding collaboration with the Langenheim Brothers’ American Stereoscopy Company, acquiring more than 3,000 glass slides for his hospital. 32 But unlike asylum-keepers who used photography to document illnesses and disorders, Kirkbride’s embrace of this new medium focused on patients’ treatment and benefit. He prohibited photography of his patients, with respect for their privacy. The photos and magic lantern shows were “for patients, not of patients.” In this regard, his practice stands opposed to the panoptical tendencies of 19th-century institutions critiqued by Michel Foucault. 33
The hospitals were pragmatically conceived as self-sustaining havens, offering dignified places for the placeless.
Kirkbride Plan hospitals complicate Foucault’s critique in other ways. While the hospitals’ long, wide hallways were indeed intended to transform behaviors, Kirkbride emphasized the psychosocializing process of moral treatment rather than the authoritarian coercion of Jeremy Bentham’s Panopticon. 34 In recent years, historians of Kirkbride hospitals have investigated “the messy slippage between the shape of a place and how it was really used.” 35 Although conditions in many of these asylums became truly dystopian, as we’ll see, close readings of the form and performance in Kirkbride Plan hospitals, especially in the early years, show that characterizing them as instruments of social control “oversimplifies the intricate relationships among building types and building uses, intentions, and practices.” 36
To be sure, there were contradictions. Moral treatment required that patients be removed from their families, who were considered a primary source of psychological disturbances. To inspire confidence, the hospital was carefully arranged as a home-like environment while also providing the structured environment and daily rhythms believed necessary for recovery. 37 Overlaid on the Linear Plan, these traces of domesticity produced an “inconspicuous confinement,” in which “architectural elements provided comfort and security without ‘the appearance of a place of confinement.’” 38 Tensions between a familial atmosphere and the emergent realities of modern institutional living were inherent to Kirkbrides, the product “of a complex interaction between the world of ideas, the reality of the asylum environment, and the lived experience of that environment.” 39 Still, the Kirkbride hospitals were focused more on the control of optics — of appearances and perceptions — than panoptical control. Embodying Enlightenment Quaker beliefs in the therapeutic powers of architecture, beauty, nature, science, and respectful care, the hospitals were pragmatically conceived as self-sustaining havens, offering dignified places for the placeless. 40

Just as important as the architecture, however, was the social program. Although these psychiatric hospitals are now called Kirkbrides, they owed their rapid spread to the relentless efforts of Dorothea Lynde Dix, without whom “the American asylum system as we know it would not exist.” 41 A social reformer who campaigned for decades to improve the lives of prisoners, the poor, and the indigent mentally ill, at a time when women were barred from politics and “could not even speak in public,” Dix founded the first Kirkbride hospital in Trenton, New Jersey, and she went on to influence the creation or enlargement of at least thirty others. 42 She mustered donations of land and finances, crafted persuasive “memorials” to be delivered to state officials and assemblies, and regularly circumnavigated the country to rally support for psychiatric care. 43
Just as important as the architecture, however, was the social program.
Described by Kirkbride near the end of his life as “my most valued and honored friend,” Dix had the respect of AMSAII’s superintendents, although she was capable, too, of inspiring their fear. One doctor wrote, “To have Miss Dix suddenly arrive at your asylum … and find anything neglected or amiss, was considerably worse than an earthquake.” 44 Historian Sonya Michel observes that “Dix acted as a kind of ventriloquist for the insane,” giving voice to their suffering even as her own words were spoken indirectly by male representatives, since women could not speak directly to legislative bodies. “By furnishing an array of facts and an indictment,” Dix “quickened the public conscience to action.” 45
Although these psychiatric hospitals are now called Kirkbrides, they owed their rapid spread to the relentless efforts of Dorothea Lynde Dix.
Her crusade on behalf of the indigent insane began in earnest in 1841, when she visited asylums, almshouses, and prisons throughout Massachusetts. She wrote her first successful memorial to the state legislature in 1843, resulting in a bill to expand the asylum in Worcester. Emboldened, Dix then visited asylums and prisons from Nova Scotia to New Orleans. Following her success at Trenton in 1845, she stated: “I have traveled more than ten thousand miles in the last three years. Have visited eighteen State penitentiaries, three hundred county jails and houses of corrections, more than five hundred almshouses and other institutions, besides hospitals and houses of refuge. I have been so happy as to promote and secure the establishment of six hospitals for the insane, several county poorhouses, and several jails on a reformed plan.” 46
Traveling alone — a formidable challenge at the time — Dix visited southern States during the winter and northern States and frontiers during the summer, and she ventured multiple times to Europe. She met with Pope Sixtus VI at the Vatican, to whom she conveyed her admiration for the asylums she had visited in Constantinople and her dismay at those she encountered in Rome. During the Civil War, Dix was appointed Superintendent of Army Nurses for the Union, establishing new standards for training and professionalism while treating both Confederate and Union soldiers. The last several years of her life were spent in a specially designed suite in the hospital she had founded in Trenton, which Dix described as her “first-born child.” 47

Building a Kirkbride hospital often created communities within and around it. Constructed with local materials — from stone, bricks, and concrete quarried or produced on site or nearby, and with lumber harvested from old-growth forests — the structures developed symbiotically with neighboring towns, stimulating their economies and civic identities. Fledgling towns and cities competed for the opportunity to have a Kirkbride in their backyards, with its promise of jobs and state funding.
Fledgling towns and cities competed for the opportunity to have a Kirkbride in their backyards, with its promise of jobs and state funding.
And even as the hospitals manifested a utopian confidence in the power of architecture to restore mental wellbeing, they also served a more pragmatic agenda. In the 1840s, when AMSAII was formed, the medical profession in the United States was in its infancy, and trained doctors sought to establish credibility amid the popularity of mesmerists, charlatans, and assorted nostrums. 48 A Kirkbride hospital, with its awe-inspiring size, layout, ornamental detailing, and technological innovations, instilled confidence in patients, families, and (initially) the taxpaying public.
The prospects for comprehensive mental health care in the United States reached their zenith in September 1854, with the publication of Kirkbride’s treatise and Congressional approval of the Bill for the Benefit of the Indigent Insane, an ambitious piece of federal legislation that Dix had championed through six years of political turbulence and escalating tensions over slavery. Modeled after land grants that had been used to develop public infrastructures for education and transportation, the “Dix Bill” (as it was popularly known) requested the sale of five million acres of the public domain, to be proportionately distributed among the 30 states according to their respective populations of mentally ill. Undaunted by the initial failure of this bill in 1848, Dix had raised her request to 12,250,000 acres (20,000 square miles), of which 2,225,000 acres would benefit the blind, deaf and dumb. (For scale, this would be an area “nearly three times the size of the State of Massachusetts.”) 49
In 1854, President Franklin Pierce vetoed the Dix Bill, which would have set aside 20,000 square miles of land to build a national infrastructure for mental health.
For five political cycles, the Dix Bill gained partial support in either the House or the Senate, only to be deferred to next year’s session. Finally, in September 1854, it passed both the U.S. House of Representatives and the Senate. Only President Franklin Pierce stood in the way of its ratification. Regarded today as one of the most inept presidents in American history, Pierce was an anti-abolitionist Northerner who did too little to stop the nation’s slide into the Civil War, and too much to stop its economic and social development, by opposing funding for infrastructure projects like canals and roads. 50 True to form, he vetoed Dorothea Dix’s proposal to build this vital national infrastructure for mental health.
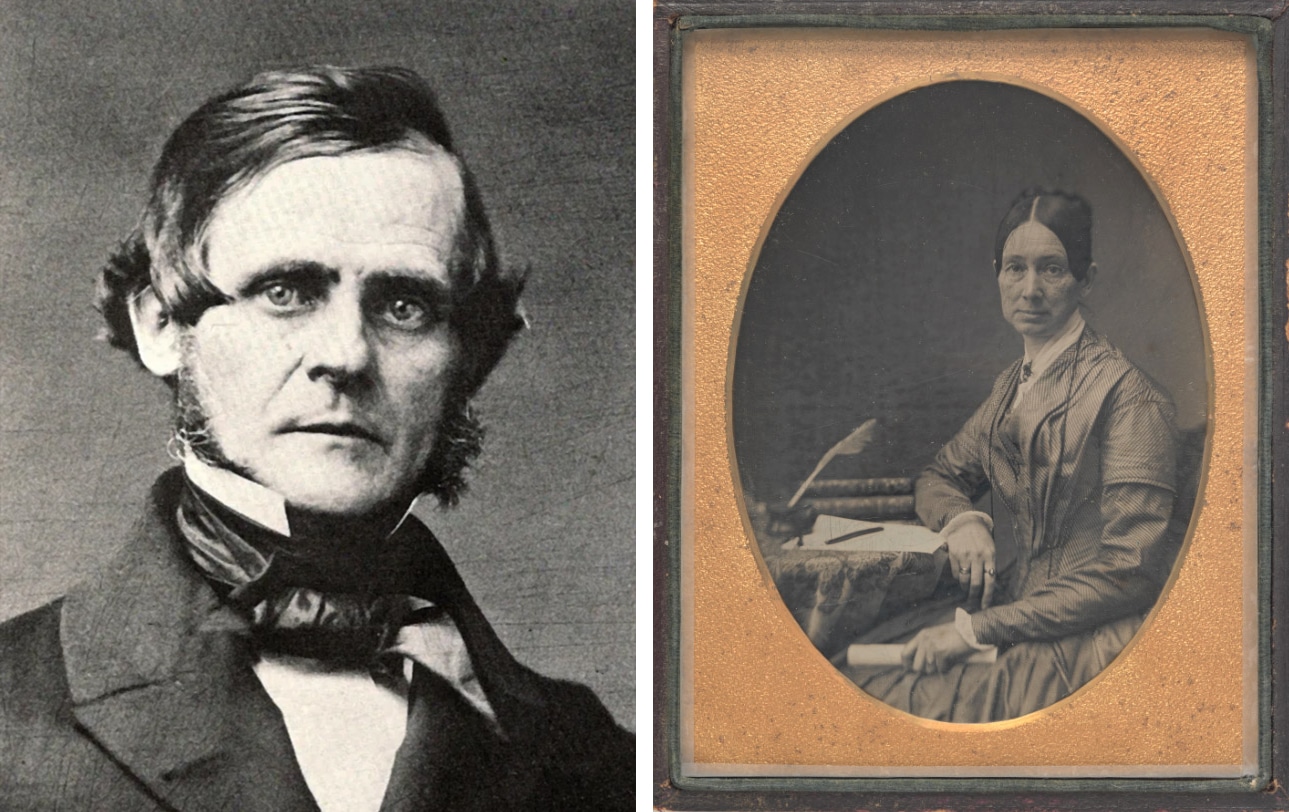
Dr. Kirkbride, a staunch advocate who had corresponded with Dix throughout, wrote to her: “Is it possible, that the President can really think of vetoing your bill? If he does, ought he not to expect to see the ghosts of insane people around his bed at night, as long as he lives?” Pierce’s veto took many by surprise. Unable to rally a two-thirds vote to overturn the veto, Dix wrote that the bill was “killed by a poor, base man in power.” 51
The architect of Pierce’s veto was in fact Jefferson Davis, the Secretary of War, who convinced the president that federal oversight of a national mental healthcare system encroached on states’ rights. Davis, soon to become President of the Confederacy, was little concerned about providing better care for the insane; his aim was to protect the southern institution of slavery. Ironically, congressional support for the Dix Bill reflected unified support among northern and southern states for a federal system of mental health care, thanks to Dix’s strategic efforts. The failure to abolish slavery at an earlier point in U.S. history thus led not only to a Civil War — with catastrophic implications for mental health across the nation — but also a closing of this window for creating a comprehensive, nationwide social and physical infrastructure for mental healthcare.
This is a defining turn in American history, in how we understand our obligations to one another, and how we formalize those social bonds through built works.
We don’t know if the federal system envisioned in the Dix Bill would have been any more successful than state-run asylums, but we do know what happened after the veto. Kirkbride Plan hospitals figured prominently during the first 50 years of mental health care in the United States, but they suffered from inadequate funding and inconsistent management. As some states began to align their asylums with penal systems, knitting punishment and stigma into the public imaginary of mental illness rather than patient-centered treatment, even those hospitals that remained focused on providing conscientious care were soon disabled from their capacity to deliver on their initial promise.
This is a defining turn in American history, in how we understand our obligations to one another, and how we formalize those social bonds through built works. We are indeed haunted by it.

Phantoms
If the Kirkbride Hospitals are haunted, they are haunted … by the difference between how history is conceived and how it plays out.
— Colin Dickey, 2016
It is useful to consider hauntology as a critical method for exploring alternate histories and what might have been. In Merlin Coverley’s words, “we may be haunted both by a past that refuses to be laid to rest and the promise of a future that refuses to be extinguished.” 52 Distinct from terms such as retro and nostalgia, which reflect an obsessive consumption of the past, hauntology points to the present and future, enabling us to engage with specters that may be difficult to face, personally and culturally.
Kirkbride hospitals — “insane asylums,” in general — have entered the popular imagination as haunted places, decrepit buildings that loom on the edge of town and radiate spooky energy. Some people are afraid of them, or of the patients who would inhabit them today. This haunting may start with painful memories of personal or family experiences with mental illness that may have been deeply stigmatizing.
Five percent of adults, and a higher number of children and teenagers, have a serious mental illness.
Yet the National Alliance on Mental Illness reports that one of every five U.S. adults experiences mental illness, and one of every six youths aged 6 to 17 experiences a mental health disorder. 53 Further, five percent of adults, and a higher number of children and teenagers, have a “serious mental illness,” with rising rates of eating disorders, self-harm, and suicide among youths who are experiencing unprecedented pressures from social media and isolation. 54 Although many are in treatment, there is no comprehensive national plan for care, and very few have access to residential facilities where they might heal, in voluntary seclusion, before returning to the world. Although a National Suicide and Crisis Lifeline was established in 2022, it is just the first part of a continuum of care that should include “a person to call, people to come, and a place to go,” as Thomas Insel, former head of the National Institute of Mental Health, summarizes. “We need places like crisis-stabilization units, opportunities for people to spend maybe 23 hours, maybe seven days, to be able to recover from whatever the acute crisis is.” 55 In a world facing intensifying disasters, pandemics, social and political unrest and injustices, support of mental wellbeing and its social and physical infrastructures must be a foremost concern.
Although many are in treatment, there is no comprehensive national plan for care.
While statistics suggest more people are experiencing disorders and mental illness, this may also reflect increasing candor and willingness to seek help. While many people are understandably averse to discussing the haunting histories of psychiatric facilities, perhaps “the language of ghosts,” as Dickey puts it, “has become an important (if abstract) way of talking about architecture and place.” 56 We are all haunted by the lost utopianism of an earlier era, and the promise of a comprehensive system of mental health care that the buildings embody. But hauntology asks us to consider the Kirkbrides from a different vantage. These buildings can help us think through social problems that are still with us, “remapping history to find paths-not-taken” and resurrecting “the future inside the past.” 57
Very few have access to residential facilities where they might heal, in voluntary seclusion, before returning to the world.
Looking back to look forward, we explore historical patterns and undercurrents, “forks in the road where things might have turned out differently, moments when new futures might have come to pass.” 58 We open up and undo historical narratives through close readings, listening for voices that have been marginalized, if not deliberately suppressed and erased. In so doing, we may uncover unrealized projects that might yet come to be. This deeper understanding of Kirkbride hospitals and their complex histories may reveal new ways the buildings can contribute to the local and regional communities they have been part of for the past century and a half, while informing a candid reflection on current crises.

One lesson here is about the limits of architectural determinism. Although buildings may offer settings that are conducive to healing, they do not in and of themselves heal us or change our behaviors. And regardless of best intentions or persuasive rhetoric, places designed for the public good — especially buildings such as asylums — cannot produce beneficial outcomes without sustained social and financial support. 59 When state asylums were constructed, it was assumed they would be the recipients of an ongoing, systemic program of care. The staged scenes in Victorian photographs and postcards at Kirkbrides offer genteel visions of idyllic retreat and hypernormality, with golf outings, croquet, carriage rides, garden pavilions, resident brass bands and costume balls, yet with time this became less and less the reality for patients. Despite their builders’ ambitions and the generosity of the designs, Kirkbride hospitals suffered from abysmal overcrowding. With reduced public funding, conditions at the hospitals soon began to deteriorate and by the end of the 19th century many were mere shades of their idealized selves.
After the Civil War, AMSAII responded to emergency conditions by raising the recommended occupancy of an asylum building from 250 patients to 600.
Although Dr. Kirkbride emphatically prescribed a scale of 200 patients per state hospital and an absolute maximum of 250, a recommendation that AMSAII formalized as policy in 1851, state hospitals were often oversubscribed at the outset. When Massachusetts’s Taunton State Hospital opened in 1854, it had 330 patients — 32 percent above the designed capacity — and the staff was immediately overtaxed. Likewise, Northampton State Hospital was designed for 200 patients, yet even before its opening, the state mandated an increase to 250. Unfortunately, the foresight with which the Kirkbride Plan preempted overcrowding in individual patient rooms did not anticipate the transformation of its generously proportioned corridors into improvised dormitories, which became the (inevitable) solution at state-run facilities for superintendents who were not permitted to deny admission. 60
The overcrowding was soon worsened by the atrocities of the Civil War, which shocked both the public and its institutions. Diagnostic terms did not yet exist for the psychological repercussions of the slaughter veterans experienced on the battlefield, or the collateral trauma to their relatives and civilians at large. 61 The nation could not even accurately count its dead. Historians in 2011 reported “the war touched more lives and communities more deeply than we thought, and thus shaped the course of American history in ways we have not yet fully grasped.” 62 As the war ended, industrialization and the rapid expansion of railways facilitated the construction of larger and larger psychiatric hospitals for the tens of thousands citizens directly and indirectly traumatized. 63 In 1866, AMSAII responded to these emergency conditions by raising the recommended maximum occupancy of an asylum building from 250 patients to 600, shattering its 1851 proposition.
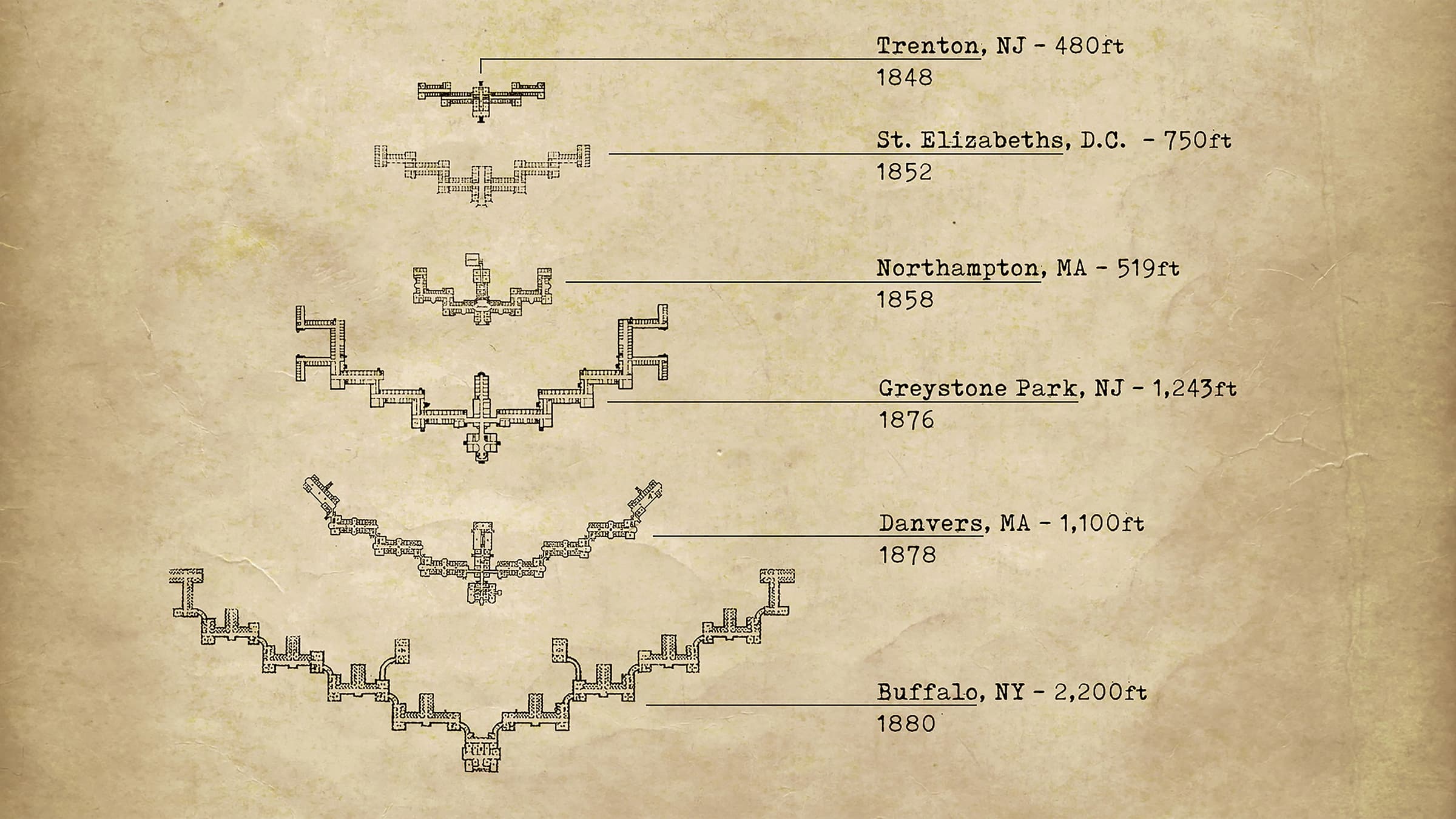
While Dr. Kirkbride strongly protested the new recommendation, he urged that if any new facilities were created for 600 patients, they should be built as two separate structures for female and male patients, capped at 300 occupants each, under different superintendents. Although a few sites (at Kalamazoo and Indianapolis) did follow this advice, most opted to add smaller “cottage style” structures incrementally, as growth demanded. Such cottages had been proposed within AMSAII as early as 1855, and they gained support with a younger generation of superintendents as population pressures mounted. 64 Kirkbride’s concession reflects a yawning loophole in the earlier guidelines, which recommended the maximum occupancy for one building, though no limit for the overall population of multiple structures on the same campus. In the wake of further national traumas, including the Panic of 1873, older hospitals sprouted additional wings, and new and increasingly massive Kirkbrides and cottages were built as rapidly as possible, at times side-by-side, as at Kankakee, Illinois, in 1878. Patient populations escalated into the thousands, overwhelming the capacity of buildings and staff to perform as planned. In sum, as Carla Yanni observes, the Kirkbrides “were never given the chance to live up to the dreams of their builders.” 65
Hospitals that had been designed to return patients to the world were now filled with chronic residents, often involuntarily confined.
With increasing populations, the recovery rates reported by state institutions became suspect. While Dr. Kirkbride was acclaimed for his successful treatment rate, he led a private hospital where he could more directly influence outcomes. 66 The typical state hospital superintendent oversaw many more patients and staff and had broader administrative duties. Even those superintendents considered humane and ethically principled were exposed to belligerent and litigious patients and politically-motivated government scrutiny. 67 In the 1880s, Pliny Earle, Kirkbride’s longtime colleague and also a Quaker, expressed the growing pessimism of superintendents, openly challenging AMSAII’s claims about the curability of mental illness. Earle published a series of research articles that revealed with crystalline precision how the data produced for annual reports had falsely inflated treatment rates. While such practices assuaged taxpayers and government officials in the short term, misrepresenting the effectiveness of mental health at state facilities led to serious complications. 68
During the first half of the 20th century, the majority of American psychiatric hospitals devolved into frightening dystopias.
Psychiatric hospitals became catch-alls for a broad range of misunderstood neuroses, developmental disabilities, neurological diseases and disorders, communicable diseases, modes of depression, and “aberrant behaviors.” 69 With rising patient numbers and diminishing state support, conscientious care devolved into custodial management, and many people spent the remainder of their lives at state facilities. Hospitals that had been designed to return patients to the world were now filled with chronic residents, often involuntarily confined. 70 With astonishing ease and convenience, patients were committed by their own family members, then abandoned. Elder siblings committed younger siblings over family inheritances. Husbands committed wives who suffered from what we recognize today as postpartum depression, placing their children in foster care, only to remarry within a year. Wives committed themselves to avoid spousal abuse. 71 Such behaviors compounded larger systemic failures and human rights abuses. Tales of mismanagement, misdiagnosis, and sinister malpractice proliferated. 72

During the first half of the 20th century, the majority of American psychiatric hospitals, including Kirkbrides, devolved into frightening dystopias, offering cautionary reminders of the frailties of social infrastructures, scientific hubris, and the dire consequences of depersonalizing bureaucratization. Increasingly invasive and unethical treatments with questionable medical value replaced respectful care, producing results that were at best inconclusive, and at worst permanently disabling and even deadly. Such procedures included insulin shock and chemical shock in the 1920s and 30s, prefrontal and transorbital lobotomies in the 1930s and 40s, chemical lobotomy beginning in the 1950s, and a eugenics program, involving forced sterilization of the mentally ill, that began at the turn of the 20th century and continued until 1981. 73
President John F. Kennedy sought to deinstitutionalize mental health care and dismantle state asylums.
Almost a century after Dr. Kirkbride first embraced photography in his Magic Lantern Therapy, Quaker activists used photography to expose the widespread mistreatment of mentally ill patients in hospitals their ancestors had helped create. During World War II, 3,000 conscientious objectors (Quakers, Mennonites, and Anabaptists) had been assigned to 62 mental hospitals across the United States. In May 1946, Life Magazine published photographs covertly taken by Charles Lord, a Quaker, showing the deplorable conditions at Byberry State Hospital in Philadelphia. Following so soon after the Allies’ military victory, the shocking images carried overtones of the concentration camps in Nazi Germany, puncturing the sense of American superiority and planting seeds for deinstitutionalizing mental health care. 74
Conceived to create one thousand community centers for mental health, the bill passed Congress but was stripped of federal funding.
Following a decade that saw the nation’s highest asylum population, 75 President John F. Kennedy — armed with statistical evidence of ineffective hospitals, bolstered by the advertised promise of new psychotropic drugs, and deeply influenced by the lifelong suffering of his sister, Rose, and the “unmitigated disaster” of her failed treatment at the hand of the notorious traveling lobotomist, Walter Freeman — sought to deinstitutionalize mental health care and dismantle state asylum-based infrastructures. 76 On October 31, 1963, Kennedy signed his last major legislation, the Community Mental Health Care Act. Although conceived to create one thousand community centers across the nation, the bill passed through Congress with “fatal flaws” that were never fully addressed after the president’s assassination. Despite its promise to treat and return the mentally ill to “a useful place in society,” echoing Kirkbride’s sentiments a century earlier, the bill was stripped of federal funding. It also provided no coordinated support for patients being discharged from state asylums or provisions for “preventative” mental health care. 77
It provided no coordinated support for patients being discharged from state asylums or provisions for preventative care.
“The movement to deinstitutionalize the mentally ill began from a place of humanity,” observed Washington Post reporter Ana Swanson, “but it hasn’t ended there.” 78 A 2014 report by the National Research Council found that the shutdown of large treatment facilities, coupled with the lack of resources for community treatment, resulted in a 7 percent growth in the prison population over two decades, “representing 40,000 to 72,000 people in prisons who would likely have been in mental hospitals in the past.” 79 Despite Kennedy’s admirable intentions, the Community Mental Health Care Act offers a haunting bookend to Pierce’s veto, just over a century earlier. Once again, a U.S. president played a pivotal role in the national narrative of mental health care. Once again, history did not turn out as planned.

In the wake of their decommissioning, we are now haunted by the materiality of psychiatric hospitals and the poignant images of their demolition by neglect. 80 The dispossessed furniture, suitcases, and forlorn articles of clothing. The hydrotherapy tubs, electroencephalography machines, and examination rooms, layered in dust. The scattered snowfall of medical records, recklessly abandoned without regard for patient privacy. The pencil marks of carpenters, the chisel-marks of masons, the marks left by water cannons that pocked the sandstone columns and capitals when the roof of Greystone Park State Asylum’s Central Main burned in 1930. The bricks of Oregon State Hospital, stamped with the name of the adjacent prison where they were produced by inmates. The roof trusses, beams, joists and flooring from old-growth forests of American Chestnut, White and Yellow Pine, Maple and Oak — the likes of which we will not see again. Traces of these forests are preserved — embedded — in the Kirkbrides at Athens, Buffalo, Traverse City, and elsewhere, too. 81
In the wake of their decommissioning, we are now haunted by the materiality of psychiatric hospitals.
And we’re haunted by the tangible traces of inhabitation — unselfconscious patterns of use, demarcations of defiance, and terrifying “stains” of happenstance. In a hallowed chamber of the Athens State Hospital, we see the outline of Margaret Schilling’s remains on the floor, unable to be erased after her body lay decomposing for more than a month after her disappearance in December 1978. 82 Tragedies like this register the dissonance between the early postcard images of life at a Kirkbride and the unimagined outcomes. Yanni observes that as the 20th century proceeded, policymaking was motivated by “the desire to keep patients out of institutions.” 83 This reflected a dramatic shift in public perception of the asylum, from a place of healing to a place of inevitable death — a “prison with no exit.”
On this very point, there are notable omissions in Dr. Kirkbride’s treatise. Given his attentiveness to the facilities essential to a psychiatric hospital, and his detailed annual reports for the Pennsylvania Institute, why did he not include any provisions for the dead and dying? Neither morgues nor cemeteries are mentioned in either edition of the treatise, and the words “dying,” “dead,” or “death” do not appear, despite the fact that many chronic patients would remain at the hospitals for decades, never to be retrieved by their stigmatized families, even after the end of their lives. 84
There are tens of thousands of unclaimed dead in cemeteries and columbaria at psychiatric hospitals, including many who remain unidentified.
We may speculate that Kirkbride avoided the subject in 1854 so as not to undermine political support for asylum construction. The taxpaying public was being asked to spend generously to cure the mentally ill through these hospitals; why should anyone die at one? Yet, as years passed, the number of chronic patients swelled, with entire hospitals dedicated to their needs, including the Kirkbride at Willard, New York, the first of its kind, which opened in 1869. 85 Regardless of his humane rationale for opposing Willard, Kirkbride had ample experience and opportunity to address the issue when his expanded treatise was published in 1880, and to offer pragmatic recommendations that might have helped prevent the situation at Fergus Falls State Hospital (1890), one of the later and larger Kirkbrides, where a basement room under one of the occupied patient wards was used as a makeshift morgue for a quarter century. 86
This is a haunting in the most literal sense. Across the country, there are tens of thousands of unclaimed dead in cemeteries and columbaria at psychiatric hospitals, including many who remain unidentified, their records lost forever or withheld by state agencies due to antiquated privacy laws and practices. Between 1890 and 1968, approximately 3,200 dead were interred at Fergus Falls, in graves marked only by a number. Thousands more were buried in a similar fashion at two other Kirkbrides in Minnesota, St. Peter and Rochester, and many other asylums across the United States. In New York state alone, “more than 55,000 psychiatric patients lie in unmarked graves.” 87


Other hauntings are no less appalling. Occupational therapy was integral to moral treatment, but as years passed and state funding ratios declined, the line between therapy and unpaid labor grew blurry. In the early years at Fergus Falls, “occupational therapy” included building pine-box coffins for deceased patients, an activity of questionable mental health benefit. At Willard State Hospital, one resident dug almost a quarter of the 5,776 graves over three decades, despite exhibiting “no symptoms of mental illness and taking no medication” for the last decades of his life. People like Lawrence Mocha were kept at asylums simply “because they were decent workers.” 88 The Fair Labor Standards Act prohibited the worst abuses of this practice after 1938, but that did not change the experiences of previous generations of patients. 89
Before asylums, the mentally ill were often kept in jails and prisons; 150 years later, this is still the case.
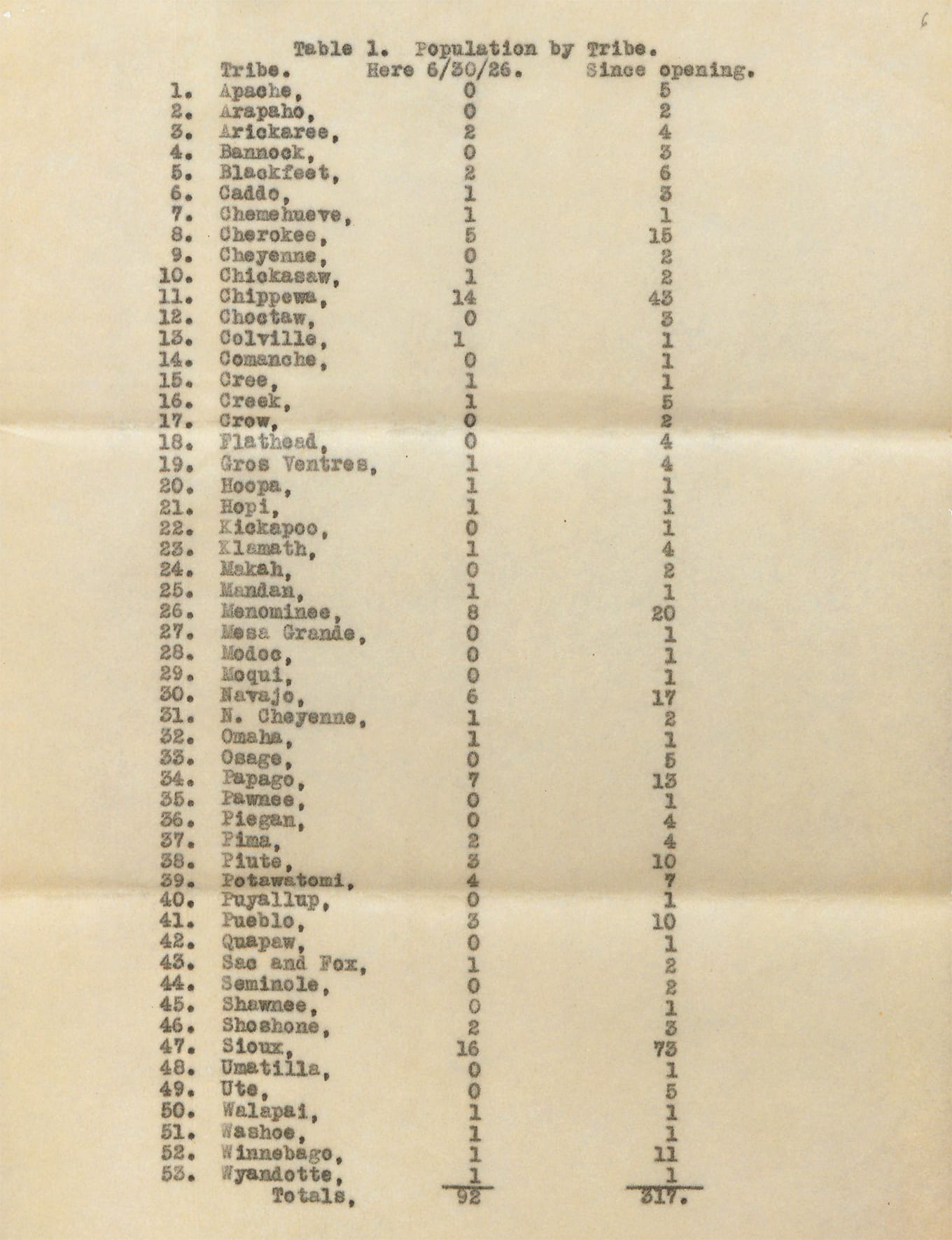
Did Kirkbride and his colleagues interrogate the ethics at southern asylums in the 1850s, where mental health care bordered on enslavement? Did they sufficiently object to the pseudoscientific “mental disorders” of drapetomania (the desire to flee slavery) and dysaesthesia aethiopis (the habit of laziness and “rascality” of resisting forced labor), which Confederate physician Samuel A. Cartwright concocted to commit and punish slaves and recently freed slaves at asylums that were essentially work camps — even after the Civil War had ended? 90 As a Quaker, would Kirkbride have been haunted by the use of St. Elizabeths as a federal repository for rebellious, non-conforming Indigenous Americans from all corners of the country, who were separated from their tribes under false pretenses and imprisoned? 91 From the mid-19th century, asylums have been used for racial profiling and suppression, and the interweaving of mental illness and incarceration in the U.S. remains a haunting narrative. 92 As reported by the U.S. Department of Justice in 2022, “half the people in U.S. jails and over one third of the population of U.S. prisons have been diagnosed with a mental illness.” 93 Before asylums, the mentally ill were often kept in jails and prisons; 150 years later, this is still the case.
With these many phantoms in mind, one wonders what changes Dr. Kirkbride might have made if he were able to consider his treatise a third time.
Afterlives
The power of architecture and what is called ‘the built environment’ is that few see it for what it is: a form of education.
— David Orr, 2008
No doubt, the doctor would be overwhelmed by these questions, much as the American public has been unable to fully reckon with them since the nation’s founding. However honorable their intentions, Thomas Story Kirkbride, Dorothea Dix, and their colleagues were among the many “unwitting builders of haunted houses” that include the nation’s asylums and prisons. 94 Reconciliation begins with attending to the phantoms that haunt these sites — whether the buildings have been demolished, are currently abandoned, or still in use today — and listening closely through the traces that remain. The Kirkbride hospitals testify to a cultural past — traumatic violence inflicted through war, genocide, and enslavement; a desire to suppress and control non-conformist behavior; and an outright refusal to support people with mental illness — that haunts our present and future.
Not only are we haunted by the Kirkbrides and their complex histories, but we ourselves haunt them.
Sharing ancestry with the author of the preeminent 19th century treatise on asylum design and management is both humbling and disquieting. My intention here is not to further a hagiography of Dr. Kirkbride, whose contributions have been thoughtfully parsed by others. 95 Nor is it to villainize or vindicate the buildings, or the therapeutic ideals they manifest. With devastating eloquence, Kirkbride Plan hospitals demonstrate how one generation’s earnest dreams — embodied through the built environment — can lay the foundations for dystopia. As I have come to see, not only are we haunted by the Kirkbrides and their complex histories, but we ourselves haunt them. We probe in our minds what might have been, had circumstances played out differently, and we imagine what might yet be, if we are able to find new purposes for the structures that remain.
Today, there are 35 extant Kirkbrides — fewer than half the original number — in varying states of integrity, use, need, and neglect. Since the deinstitutionalization of mental health care, some Kirkbrides have been replaced by big-box stores, and others by empty lots. 96 Many people would be delighted to demolish the remaining buildings, either to repress a difficult history, or to develop the land beneath them for their personal or political gain. Yet debates about whether to keep or destroy these buildings hinge on matters deeper than the development value of the site. Far from useless, these large, old, structures offer significant benefits, and there is a growing list of successful examples of adaptive reuse. 97

Following my grandparents’ fascination with historical traces embedded in a decaying urban fabric, I explore Kirkbride hospitals as palimpsests that reveal complex, layered histories extending to the present, as we struggle to support mental illness across all ages. And while I share my grandfather’s ambivalence about Quaker colonial histories and my family’s participation in them, including these hospitals, I also share his commitment to preserving that fabric as material for our improved understanding, renewed hope, and future dreaming. Shown here: Hudson River State Hospital, Poughkeepsie, New York, a National Historic Landmark currently at risk. [Lisa Marie Blohm]
Fergus Falls Psychiatric Hospital, Fergus Falls, Minnesota, an at-risk Kirkbride listed on the National Register of Historic Places. [Robert Kirkbride]
Kirkbride Hall, at Traverse City State Hospital (now The Village at Traverse City Commons), adaptively reused and NRHP listed. [Robert Kirkbride]
Ventilation towers at Traverse City State Hospital. [Robert Kirkbride]
Oregon State Hospital, Salem, Oregon, NHRP listed and an active psychiatric hospital. [Robert Kirkbride]
Weston State Hospital, a preserved National Historic Landmark with 70,000 visitors per year. [Robert Kirkbride]
Buffalo State Hospital, a partially adapted National Historic Landmark under continuing redevelopment. [Robert Kirkbride]
East (men’s) wing, Buffalo State Hospital, used as children’s wing from 1961 to early 1970s. [Robert Kirkbride]
Detail of original stenciled ornamentation and multiple layers of overpainting at Buffalo State Hospital. [Robert Kirkbride]
West (women’s) wing, Buffalo State Hospital. [Robert Kirkbride]
Yellow parlor, west (women’s) wing, Buffalo State Hospital. [Robert Kirkbride]
Ceiling of patient room, west (women’s) wing, Buffalo State Hospital. [Robert Kirkbride]
Athens State Hospital (now The Ridges), NRHP listed and under continuing redevelopment. [Robert Kirkbride]
Outermost north (women’s) wing of Dayton State Hospital (now 10 Wilmington Place). [Robert Kirkbride]
Central main building at Hudson River State Hospital, with the author and architecture students from an adaptive reuse studio at Parsons School of Design, Spring 2024. [Yvonne Laube]














Among other possibilities, Kirkbride buildings and campuses have potential to provide more affordable housing, which is the foundation for mental health for many individuals. Our collective imagination and resourcefulness are reflected in our capacity to find new uses for the built environments we inherit. 98 In an era of scarcity, with the ecological imperative to repurpose our existing built environments, the erasure of these historically layered, three-dimensional documents is an unacceptable waste of embodied energy and cultural memory. 99
Our collective imagination and resourcefulness are reflected in our capacity to find new uses for the built environments we inherit.
We can’t learn from our past to envision different futures without things to think with. 100 Other cultures have adaptively repurposed buildings with difficult and contested pasts, as a way of living with and learning from their histories. Can’t we? Many people today do not share the stigmas about mental illness held by previous generations. 101 They don’t seek to erase or bury the past but to engage with it, learn from it, to challenge and transform our histories and ourselves. We must find new lives for these remarkable structures, which offer tangible lessons, both architectural and cultural. If we don’t, we may someday be haunted not only by our collective failure to care for people who are suffering, and the memories of those who suffered before them, but also by our collective failure of imagination in designing a better world. These are the phantoms that should frighten us most.


{kind=link}
{kind=link}
If you would like to comment on this article, or anything else on Places Journal, visit our Facebook page or send us a message on Twitter.